Spina Bifida CIC booklet

Spina Bifida CIC booklet
A practical guide for nurses and health workers
to do clean intermittent catheterization (CIC)
version 26/2/2018
Table of Contents
Importance of CIC in Spina Bifida children 3
What to do before starting CIC 5
What to do when starting CIC 6
What to check before starting Oxybutynin 10
Dose of intravesical Oxybutynin 11
What to do in case of a urinary tract infection 12
What to do on follow-up visits 13
Example of a urine volume chart 14
When you have problems, what can be wrong 15
Importance of CIC in children with Spina Bifida
Clean Intermittent Catheterization (CIC):
-
helps to avoid urinary tract infections
-
helps to avoid dangerously high bladder pressure and kidney damage (keeps bladder and kidneys in a healthy condition)
-
is necessary to become (socially) continent
IMPORTANT
-
Tell the parents that CIC does not harm the genitals or affect fertility
-
but that CIC helps to avoid bladder and kidney damage!
-
If there is also constipation, CIC will need to be combined with bowel training from the age of 2.
(see bowel booklet)
When to start CIC
-
In the case of bladder retention: seen by inspection of the abdomen and a bladder palpable up to the umbilical level
-
In the case of more than one proven urinary tract infection
-
A desire to become continent
What to do before starting CIC
-
Assess how the child is peeing:
-
is there urine retention (by feeling)
-
is the child dribbling when handled
-
does the child pee with a high pressure
-
Do a urine analysis using a dip stick (Combur-2 sticks)
Analyze twice weekly when the child is an in-patient and at every visit in the outpatient clinic
-
Plan a renal / bladder ultrasound if possible to screen for high bladder pressure
-
In the case of a proven urinary tract infection start nitrofurantoin or co-trimoxazole for 5 days and control the urine after treatment (see page 8)
-
If the child is a boy, assess the need for circumcision
-
If a second infection is proven, start CIC
What to do when starting CIC
-
Give a clear explanation of the importance of CIC to parents and children.
-
Make sure you have all the material necessary.
-
Use the largest size of catheter that can enter the urethra without force.
-
Do a good CIC and empty the bladder completely.
-
Instruct the parents how to do the CIC themselves and show them how to assess the urine:
|
Clear |
OK |
|
No smell |
|
|
Cloudy |
Infection |
|
Bad smell |
|
|
Blood in urine |
-
Instruct the parents how to note the volume removed at every CIC on a special volume chart (see volume chart).
-
Start with CIC 3 times (3 times is enough to reduce infection) but increase frequency to
5 times a day as soon as possible.
If necessary and if CIC technique is well known by the parents, start Oxybutynin.
(see manual of Oxybutynin)
Material
-
Silicone Catheters, no latex to avoid allergies
-
Lubricant for boys (KY Jelly, Paraffin). If not available, try water.
-
Colorless transparent recipient to collect the urine
-
Non-sterile materials to wash genital area
-
Water and soap to wash hands
-
Latex free gloves
-
Use the widest catheter that can enter the urethra
For boys: start with CH 8 short for babies and toddlers. CH 8 Long afterwards.
For girls: always use short.
How to do a good CIC
CIC is only well done when the bladder is totally empty after CIC. Even a few drops of urine left in the bladder can cause a bladder infection.
-
Wash your hands and use latex-free gloves (parents only have to wash their hands).
-
Clean the genital area with water and soap:
-
Once a day, after every soiling or emptying the bowels
-
Always wash from front to back to avoid feces from reaching the urethra.
-
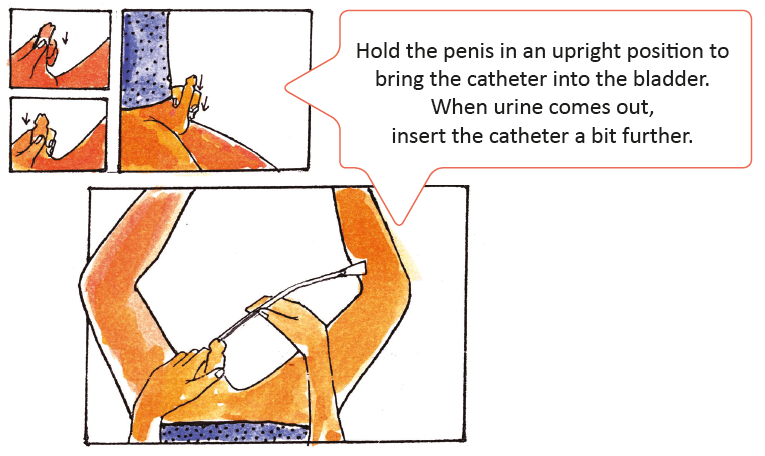
Insertion of the catheter
-
Use the widest catheter that can enter the urethra without forcing.
-
For Boys: place lubricant on the back of the hand and spread out on the tip of the catheter. If lubricant is not available, use water.
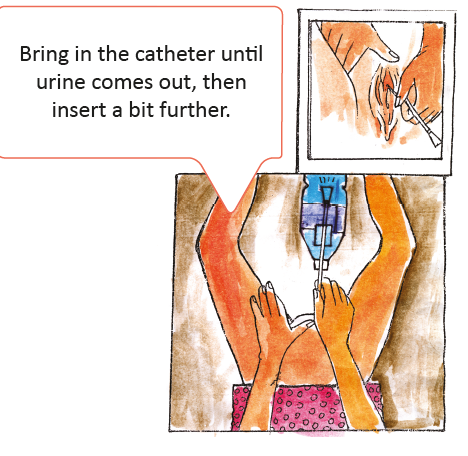
For Girls: spread the labia so that to urethra is clearly visible.
-
Put the catheter into the urethra until urine comes out.
-
Advance the catheter a bit deeper to make sure both holes are into the bladder.
-
Capture the urine in a transparent recipient and control if the urine is clear/cloudy.
-
Let the urine flow. When the urine stops to flow, apply pressure above the pubis.
-
Withdraw by slowly turning the catheter downwards.
-
Wash your hands
To prevent infections, the bladder needs to be completely empty after each catheterization.
 To check after CIC
To check after CIC
-
Measure the urine volume obtained and note it on a chart
-
Teach the parents how to measure urine volume at home. Parents have to note the volumes 3 days before coming to the next consultation
-
When you always measure small amounts of urine DO NOT stop CIC but start to use Oxybutynin (the bladder muscle is too active)
-
When the urine smells and is cloudy, the urine is infected. (see page 12 about infections)
Clean and store catheters
-
Rinse the in and outside of the catheter with water
-
Shake off the remaining water. Leave it to dry in the sun when possible.
-
Store in clean piece of cloth
Why to start Oxybutynin
Oxybutynin prevents bladder overactivity
When to start Oxybutynin
-
When the urine volumes are always very small
-
If there are still urinary tract infections after starting CIC
-
To improve social continence
When to stop Oxybutynin
There is no reason to stop Oxybutynin,
the child will require to take it his/her whole life.
What to check before starting Oxybutynin
-
Be sure that parents and/or the child are able to do a good CIC
-
Assess the size of catheter; the widest size which enters the urethra easily, without forcing is the best
-
Check the urine for infection (cloudy and bad smell) by using urine control sticks (urine-10 sticks)
-
Start to use 0.2 mg Oxybutynin/kg bodyweight BD (see page 11)
-
Measure the volumes and assess whether they are increasing
-
The child should be dry for longer periods in between CIC and/or bigger volumes should be obtained
IMPORTANT
The solution of Oxybutynin has to be stored in the dark!
Put it in a towel and keep it in a closet!
What to do in case of urinary tract infection
-
Infected urine is cloudy and has a bad smell. Teach the parent that they have to assess this at home
-
When in doubt, you can assess leucocytes level using a dip stick (Combur-2 sticks).
-
Ensure a good catheterization technique during the first 24 hours and encourage the child to drink extra water
-
Do not stop the Oxybutynin
-
Empty the bladder completely by holding the child in an upright or standing position (if possible) for 1 or 2 times a day
-
If possible, use a wider catheter (bigger CH)
-
After 24 hours you have to assess the urine again using a leucocytes stick (Combur-2 sticks)
-
If the stick is negative, the infection has cleared. If it is still positive you can start nitrofurantoin or trimethoprim/ co-trimoxazole for 5 days. It’s not necessary to treat all infections with antibiotics, do a good CIC technique ensuring to completely empty the bladder:
Doses
Newborns / 6 weeks to 5 months:
Nitrofurantoin (not before 3 months) 1mg/kg x 3times a day
Trimethoprim 20mg BD or Co-trimoxazole 120mg BD
6 months until 5 years:
Nitrofurantoin 1mg/kg x 3times a day
Trimethoprim 40mg BD or Co-trimoxazole 240mg BD
6 years until 12 years:
Nitrofurantoin 1mg/kg x 3times a day
Trimethoprim 80mg BD or Co-trimoxazole 240mg BD
REMARKS:
Co-trimoxazote = trimethoprim 1/5 + sulfamethoxazole 5/5
Look for the local used names of these medications
What to do on follow-up visits
-
Check the urine for infection
-
Does the child have bigger volumes of urine than before the start of Oxybutynin?
(look at the volume chart)
-
Ask the parent if the child is able to remain dry for longer periods
Remarks:
-
The urine volume chart is a very important instrument to follow the success of the treatment.
-
Explain the parents how they can measure and note these volumes.
-
They have to learn it in the hospital.
-
They have to note it on the chart during 3 days in the week before they come to outpatient clinic.
Potential problems after starting CIC
-
The child is still wet
-
Assess if there is a urinary tract infection, increase fluid intake and do a good CIC. If the infection does not clear, start nitrofurantoin or co-trimoxazole (see page 8)
-
Assess whether the frequency of CIC is adequate
-
Assess whether the child would benefit from Oxybutynin (if not already on it)
-
If the child is constipated, start bowel washout
-
If all above do not improve continence, further assessment and review by a specialist is necessary as surgery may be required
-
Still a lot of urinary tract infections
-
Check if the child uses the correct size of catheter, assess if a wider size is possible (do not force)
-
Assess if the parents perform CIC technique correctly (see page 7)
-
Assess the frequency of CIC (5 times a day)
-
Check if the child is already on Oxybutynin and if the parents give it on a regular base. Start it if necessary.
-
Assess if you have to raise the dose of Oxybutynin (see page 11)
-
Assess if the child uses bowel training and start it if necessary
-
If the infection does not clear ask the doctor for a renal and bladder echo or RX cystography, if possible, to assess for vesico-urethral reflux
-
A few drops of blood into the catheter after CIC
-
A few drops of blood after CIC does not give problems if it disappears after 2 or 3 catheterizations
-
Look if the catheter is damaged. Replace if necessary
-
If there is a lot of blood, there can be a wound inside. Ask a doctor if you have doubts
-
Problems with inserting the catheter
-
Check if you use the good size of catheter, you have to use the widest one which can enter the urethra (do not force)
-
Use lubricant for boys (girls do not need it)
-
Look if the catheter is damaged. Replace if necessary
-
If you still have problems with boys, ask the doctor to assess if there is trauma
-
Feeling pain when using Oxybutynin solution
-
The child can have a painful sensation if the catheter tip is not inserted deep enough
-
Insert the catheter deeper in the bladder before the instillation and do not instill the solution too fast

No comments to display
No comments to display